Cochrane Database Syst Rev. 2013 Mar 28;3:CD004310. doi: 10.1002/14651858.CD004310.pub3.
- h0 }1 T% M" BMegestrol acetate for treatment of anorexia-cachexia syndrome.
- F7 q1 {/ b) ]Ruiz Garcia V1, López-Briz E, Carbonell Sanchis R, Gonzalvez Perales JL, Bort-Marti S.
) a: k( @* A; [) J+ GAuthor information
' ~" a& O$ K. B$ X$ OAbstract
4 t3 I- W( |+ N" D. ]1 J, \! G TBACKGROUND:
/ x: g2 d, t3 n9 S3 g% A; y) w! NThis is an updated version of a previously published review in The Cochrane Library (2005, Issue 2) on 'Megestrol acetate for the treatment of anorexia-cachexia syndrome'. Megestrol acetate (MA) is currently used to improve appetite and to increase weight in cancer-associated anorexia. In 1993, MA was approved by the US Food and Drug Administration for the treatment of anorexia, cachexia or unexplained weight loss in patients with AIDS. The mechanism by which MA increases appetite is unknown and its effectiveness for anorexia and cachexia in neoplastic and AIDS (acquired immunodeficiency syndrome) patients is under investigation., l! s2 g" m! D F# Z" i
OBJECTIVES:
4 g0 N' L3 U+ t+ L. t# |% C7 XTo evaluate the efficacy, effectiveness and safety of MA in palliating anorexia-cachexia syndrome in patients with cancer, AIDS and other underlying pathologies.! ~7 b( L. K6 w: V U
SEARCH METHODS:
: R% t F+ C( N' i! oWe sought studies through an extensive search of electronic databases, journals, reference lists, contact with investigators and other search strategies outlined in the methods. The most recent search for this update was carried out in May 2012.1 Z% ^1 @* B# D1 U# w7 d5 z
SELECTION CRITERIA:
7 S& a- i+ I2 X1 Z9 s+ fStudies were included in the review if they assessed MA compared to placebo or other drug treatments in randomised controlled trials of patients with a clinical diagnosis of anorexia-cachexia syndrome related to cancer, AIDS or any other underlying pathology.
- ?6 B8 `; U4 EDATA COLLECTION AND ANALYSIS:
1 I8 J7 h/ ?, j3 n) I7 V2 vTwo independent review authors conducted data extraction and evaluated methodological quality. We performed quantitative analyses using appetite and quality of life as a dichotomous variable, and analysed weight gain as continuous and dichotomous variables.
' T9 H9 `8 U0 i/ SMAIN RESULTS:
3 N$ J0 E0 F5 ~4 nWe included 35 trials in this update, the same number but not the same trials as in the previous version of the review. The trials comprised 3963 patients for effectiveness and 3180 for safety. Sixteen trials compared MA at different doses with placebo, seven trials compared different doses of MA with other drug treatments and 10 trials compared different doses of MA. Meta-analysis showed a benefit of MA compared with placebo, particularly with regard to appetite improvement and weight gain in cancer, AIDS and other underlying conditions, and lack of benefit in the same patients when MA was compared to other drugs. There was insufficient information to define the optimal dose of MA, but higher doses were more related to weight improvement than lower doses. Quality of life improvement in patients was seen only when comparing MA versus placebo but not other drugs in both subcategories: cancer and AIDS. Oedema, thromboembolic phenomena and deaths were more frequent in the patients treated with MA. More than 40 side effects were studied.
. Q+ P7 [% g& _) y2 u: LAUTHORS' CONCLUSIONS:
, v* r3 M2 F- T% q& mThis review shows that MA improves appetite and is associated with slight weight gain in cancer, AIDS and in patients with other underlying pathology. Despite the fact that these patients are receiving palliative care they should be informed of the risks involved in taking MA.
' t+ K" J/ x5 c5 Q" W1 f; E7 r% N |
 汇总4月最新:临床试验招募| 小细胞
"化疗±免疫后进展了,还能怎么办?"——这是许多小细胞肺癌患者和家属的困境。
临
汇总4月最新:临床试验招募| 小细胞
"化疗±免疫后进展了,还能怎么办?"——这是许多小细胞肺癌患者和家属的困境。
临
 需要加论坛患者群的朋友们看这里
本帖最后由 青菜567 于 2024-7-22 17:38 编辑
与癌共舞小助手-29新进论坛需要进入患
需要加论坛患者群的朋友们看这里
本帖最后由 青菜567 于 2024-7-22 17:38 编辑
与癌共舞小助手-29新进论坛需要进入患
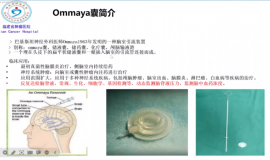
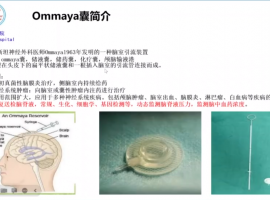 神奇的ommaya囊——学习笔记
一个神奇的装置-ommaya囊——————9.28 苗茜医生科普讲座
直播链接:https://live.
神奇的ommaya囊——学习笔记
一个神奇的装置-ommaya囊——————9.28 苗茜医生科普讲座
直播链接:https://live.
 母亲肺腺癌晚期骨转移,EGFR21突变,
母亲1970年出生,56周岁,身高163cm,体重98kg(196斤)。2025年9月23日肺炎住院,胸
母亲肺腺癌晚期骨转移,EGFR21突变,
母亲1970年出生,56周岁,身高163cm,体重98kg(196斤)。2025年9月23日肺炎住院,胸
 临床试验招募| 铂类化疗失败后的经治
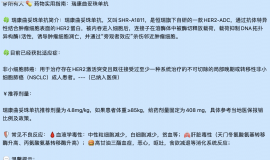
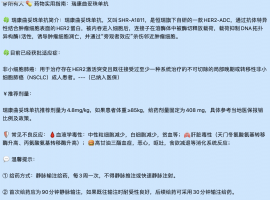
🔥 项目题目:AL8326片治疗至少接受二线治疗方案后疾病进展或复发的小细胞肺癌患者
临床试验招募| 铂类化疗失败后的经治
🔥 项目题目:AL8326片治疗至少接受二线治疗方案后疾病进展或复发的小细胞肺癌患者






 显身卡
显身卡